by George Guess, MD, DABHM
Abstract: Two ophthalmologic cases treated homeopathically are presented—iridocyclitis and central serous retinopathy. In each case core mental-emotional characteristics were essential to identification of the indicated homeopathic medicine. The iridocyclitis case responded brilliantly to Calcarea carbonica in ascending potencies, which was prescribed primarily on the basis of causation, namely stress associated with fear for financial and occupational security and a resultant cautiousness, coupled with an early tendency to pupillary adhesions (synechiae). The retinopathy case, lacking any useful symptoms relating to the pathology, responded curatively to Carcinosinum burnett, prescribed on the basis of the patient’s intense need for control in all elements of his life, as well as his fastidiousness and sympathetic, pleasing nature.
Keywords: fibrinous iridocyclitis, central serous retinopathy; psychodynamics, the importance of in homeopathic prescribing; Calcarea carbonica, Carsinosinum burnett
A Case of Chronic Recurring Iritis
Iritis, more aptly termed iridocyclitis, is an inflammation of the iris and ciliary body of the eye, causing swelling, redness, pain, lacrimation, discoloration of the iris, pupillary constriction and possibly deformation, possible hypopion, and affecting vision. Causes are variable and can include: trauma, various viral, bacterial, protozoal diseases, allergy, autoimmune diseases, metabolic disorders (diabetes, gout), and others (sarcoidosis, Behcet’s disease, etc.). Conventional treatment can include: antimicrobials, anti-inflammatory drugs, corticosteroids, antihistamines, mydriatics, immunomodulators, etc. Topical steroid treatment, if prolonged, as can be required in some cases, presents the risk of complications such as glaucoma and cataract. “Plastic iritis,” the term used to describe the case below and currently known as fibrinous iridocyclitis, is distinguished from other types of iritis by the composition of the inflammatory exudate produced, which contains more albumin and large molecules of globulin and fibrin, a consequence of increased thinness of the ciliary body’s capillary walls and which results in a thicker exudative suspension in the anterior chamber of the eye. The adhesive exudative components easily fuse the iris to the lens surface resulting in pupillary synechiae, distorting the iris. Such distortions of the iris can become permanent if the pupil is not dilated as part of treatment. Iritis can be both acute and chronically recurring, the former lasting a few weeks, the latter months and can be recurrent. Acute iritis, treated in a timely fashion, can resolve in 10-15 days often. Left untreated, iridocyclitis can result in various severe complications threatening vision permanently and even the eye itself. 1,2
Patient Presentation
June 1996 (telephone consultation)
A 45-year-old man presented complaining of recent onset of yet another bout of iritis, this time of the left eye. The iritis could affect either eye, although it predominated in the right eye, and had been recurring episodically over the past 24 years despite conventional medical treatment which largely consisted of either intraocular steroid injections or topical steroids and cycloplegics to prevent the pupillary synechiae that had a tendency to develop rapidly in his case. The recurrences had been increasing in frequency from approximately every two years to biannually more recently. An ophthalmologist seen recently diagnosed the condition as plastic iritis (an outdated term, likely indicating fibrinous iridocyclitis). At the time of this initial consultation the patient was only on mydriatics for synechia prophylaxis.
The iritis symptoms consisted of:
- Soreness of the eye and the surrounding extraocular muscles, worse touch.
- Slight photophobia.
- Headache from using the eyes, especially from reading.
- Sensation as of ‘tiny explosions’ in the eye and popping sensations.
- Sensation as of an eyelash in the eye.
- Swelling about the eye.
- In this and previous episodes marked lacrimation.
- Eye pain better from both cold and warm applications. (He disliked cold applications on his head as they made his head too cold.)
- He was averse to exertion during the flares, the eye pain being worse from walking, jarring and shaking his head. Lying down brought some relief.
The patient was a college professor and, over the years, had associated the iritis flares with work-related pressure, such as his stress-laden preparations to defend his PhD dissertation, as well as other work stress. Such periods of stress usually involved considerable reading, and, thinking that exertion of the eyes might be the cause (Ruta), I inquired as to what he considered the principal stressor. He replied that the psychological pressure was much more at play, and, interestingly, he reported that the flares occurred after having finished his work, once he felt relieved.
 Each bout brought on depression as well. The iritis was a ‘career killer’ he lamented. Originally having aspirations to a very different career, the iritis made pursuing that work impossible and he had to settle for a life in academia that, once achieving tenure, provided more financial security, especially if the disease resulted in blindness. As a consequence, he felt he had to settle for a far less interesting and less remunerative profession. Dwelling on this setback with each iritis flare left him morose.
Each bout brought on depression as well. The iritis was a ‘career killer’ he lamented. Originally having aspirations to a very different career, the iritis made pursuing that work impossible and he had to settle for a life in academia that, once achieving tenure, provided more financial security, especially if the disease resulted in blindness. As a consequence, he felt he had to settle for a far less interesting and less remunerative profession. Dwelling on this setback with each iritis flare left him morose.
His desired career would have provided excitement and kept him more engaged. By nature, he possessed a decided wanderlust and loved adventure, excitement and travel; he now felt subdued by his disease and as if time and opportunity were passing him by. Where once rather reckless, he’d become cautious and overly concerned with finances and security. He’d also once been quite passionate about politics and social justice, but now noted a distinct cooling of those passions, to his regret.
His most recent flare was preceded by anxious anticipation as he awaited word of his winning tenure at his college; soon after receiving good news and experiencing great relief, this latest flare arose. The one welcome aspect of the ailment, he confessed, was the rest that became a necessity during flares, during which he could play music, contemplate, and relax. “I look forward to that side of it.”
Fears: Some claustrophobia. He also feared losing loved ones—whenever his wife left home for a length of time, he became rather anxious about her welfare. He also feared for his children’s future, and was seriously phobic about anything tight about his neck, although he could wear a tie. He was also rather sympathetic.
Nail biting was a bad habit.
During the consultation a rather marked loquacity was noted.
Generalities: The patient was warm-natured but also tolerant of both heat and cold. Perspiration was normal. He was thirsty and possessed a strong appetite.
Food desires: salty, jello and puddings, fish, avocadoes, cheese, wine and beer, basmati rice.
Aversions: candy. He felt a bit ill from the odor of burning fat. The patient had a great love for the ocean, although no amelioration was experienced there.
Sleep: fairly normal. Position: sides, right more than left. Snored when lying on his back. Covered. No bruxism. The patient reported a very active dream life, his dreams full of romance and sex, and involving many of his female friends when younger. He also dreamt of being chased by husbands.
He admitted that he couldn’t talk to a woman without imagining what she’d be like in bed, as well as having had a few extramarital affairs.
His past history was remarkable for two outbreaks of Herpes genitalis; there was no history of other STD’s, urethritis or UTIs.
Assessment: Although cognizant of a few of the more remarkable presenting symptoms—lascivious, amorous dreams, adulterous, loquacity, desire to travel and love of adventure, phobia regarding constriction at the throat—that suggested to me certain possible highly-sexed homeopathic medicines such as Lachesis, Medorrhinum, Phosphorus, Lachesis, etc., what nevertheless most impressed me about this case was the patient’s striking anxiety about his career and financial security, the associated stress-related causation of each iritis flare (with the interesting appearance of symptoms immediately following the easing of the stress as opposedto during the height of it), plus the reported rapid development of pupillary synechiae with each iritis flare.
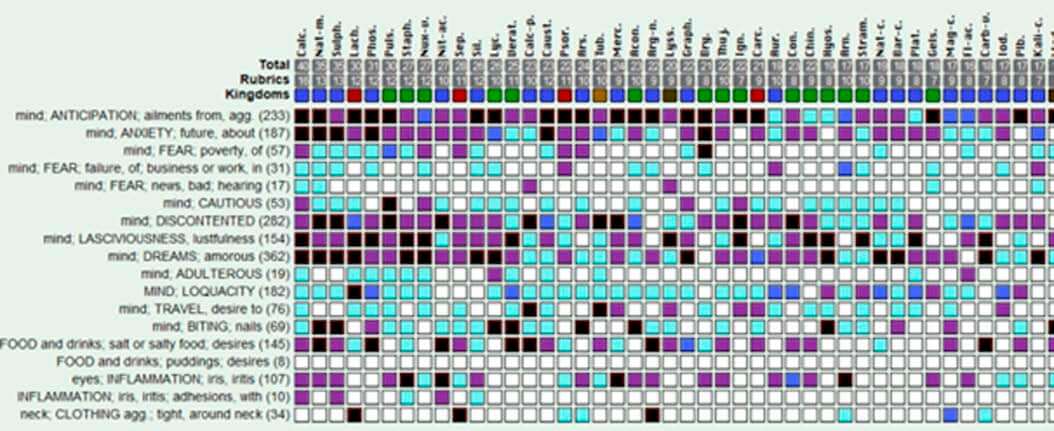
Setting aside this patient’s intemperate sexual preoccupation, coupled with certain ancillary characteristics, that suggested an underlying dysfunctional state appearing to call for a homeopathic medicine belonging to the aforementioned group, a narrowing of analytic focus to the characteristics mentioned above relating to causation, associated anxiety and fear, and eye pathology (adhesions), led me to Calcarea carbonica. As noted above, Calcarea carbonica was very well represented in the repertorization (CR 2016, MacRepertory); additionally, it has very well-recognized occupational and financial security concerns (as confirmed by such rubrics as: Anxiety about the future, Anxiety about health, Fear of hearing bad news, Fear something will happen, Fear of poverty, Talks of money, Financial loss aggravates, Fear to lose his lucrative position, Fear of failure in business or work—from MacRepertory, CR 2016 ), a tendency to cautious behavior, and, I was sanguine to find, can possess a quite strong sexual energy, even excessive. (T.F. Allen’s Encyclopedia: Sexual Organs: Male: “Sexual desire much increased. Great desire for coition . . . Excessive sexual desire, caused by lascivious fancies . . .”
C. Hering’s Guiding Symptoms: Female: “Nymphomania.”) In so settling upon that medicine, I set aside his warm-bodied physiology, especially since it wasn’t strongly emphasized. Furthermore, the materia medica of Calcarea carbonica bears a strong resemblance to this patient’s physical pathology.3
Prescription: Calcarea carbonica 6C, in liquid attenuation, with instructions to begin dosing once a day, continuing until the iritis subsided. I chose a lower potency to initiate treatment to preclude provoking a strong homeopathic aggravation.
 Case progress (summarized): Within a week, the patient reported that the intensity of his iritis symptoms began improving within 2-3 days and the condition was completely relieved by week’s end. In that he lived a distance away and was disinclined to pursue regular follow-ups, I advised that he could repeat the Calc-c 6C at the first sign of a similar stress-related relapse. He, in fact, was required to do so a few times over the course of the next two years. He contacted me when the 6C showed signs of failing, leading to the prescription of 12C, later 30C, and finally 200C for subsequent flares. Finally, after the latter potency, given at the two-year point, the iritis subsided for good, not having recurred since 1998. In the interim his health has been rather good overall but for a bout of deep vein thrombosis several years later. Whether the intensity of sexual energy previously described persists is unknown.
Case progress (summarized): Within a week, the patient reported that the intensity of his iritis symptoms began improving within 2-3 days and the condition was completely relieved by week’s end. In that he lived a distance away and was disinclined to pursue regular follow-ups, I advised that he could repeat the Calc-c 6C at the first sign of a similar stress-related relapse. He, in fact, was required to do so a few times over the course of the next two years. He contacted me when the 6C showed signs of failing, leading to the prescription of 12C, later 30C, and finally 200C for subsequent flares. Finally, after the latter potency, given at the two-year point, the iritis subsided for good, not having recurred since 1998. In the interim his health has been rather good overall but for a bout of deep vein thrombosis several years later. Whether the intensity of sexual energy previously described persists is unknown.
Central Serous Retinopathy-A Case
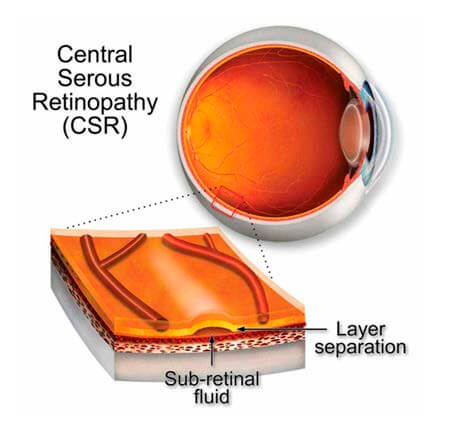
Central Serous Retinopathy (or Chorioretinopathy) [CSCR], a common and as yet idiopathic chorioretinopathy, is a serous detachment of the neurosensory retina due to sub-retinal fluid extravasation. It results in unilateral central visual loss or distortion and affects primarily white males in the 20-50 years of age range, although any gender and age can be affected. Most cases are acute and self-limited, tending to be of about 2-3 months duration, although some cases of chronic CSCR occur, presenting a risk of retinal epithelial atrophy and permanent loss of vision. Although the mechanism of pathogenesis is unclear, steroid excess, both endogenous cortisol and exogenous corticosteroids, is closely correlated with CSCR occurrence; consequently, in those cases not associated with exogenous steroid exposure “CSCR’s association with having a Type A personality seems logical given known increased glucocorticoid release with stress.”4
Many cases are simply observed, given their tendency to spontaneous resolution. Chronic progressive cases are usually addressed with photodynamic therapy. Additional more recent treatment options include subthreshold micropulse laser photocoagulation or mineralocorticoid antagonists.4
Patient presentation
April 2001
A 38-year-old businessman consulted for chronic sinusitis and central serous retinopathy (CSCR). His sinusitis consisted of nasal and sinus congestion with few to no distinguishing characteristics. When asked about his eye ailment, the only symptoms mentioned were a cloudiness of vision and a slightly skewed appreciation of colors.
He described himself as ‘edgy’ and prone to become irritated and short with his business clients. His life centered on his career, about which he was extremely perfectionistic. He sought ‘complete control’ in his work. Despite his career focus and ambition, he was very sympathetic to his clients’ situations. His was also an appeasing personality, finding it difficult to say no to others lest he feel guilty. His perfectionism was also reflected in his physical surroundings about which he was fastidious.
He was a chilly person. His sleep was restless and disturbed by thoughts of business. Occasionally he experienced bouts of panic with choking at night.
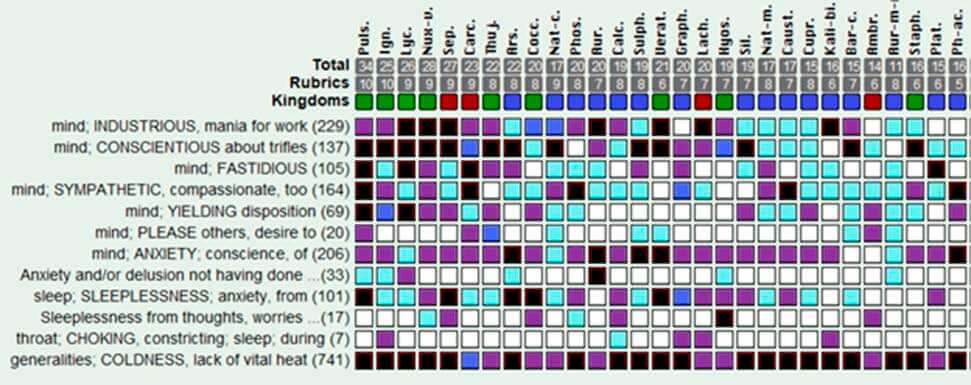
Assessment: Lacking any distinctive characteristics referable to the pathology and generalities of this gentleman, it was readily apparent that the solution to his case lay within the realm of his personal qualities, his constitution, so to speak. This was a driven individual, industrious, ambitious, fastidious, perfectionistic and clearly tightly wound with his need to control events. Such features belied the selection of such medicines as Pulsatilla, Lycopodium, and Sepia. Ignatia was a possibility, especially with this patient’s nocturnal choking, but where was the history of grief, the idealism (Mind; IDEALISTIC: 3Caust., cer-p., dysp-s., 3Ign., ignis, lyc., neod-f., neod-o., 3Plat., pras-o., sama., sama-c. – Complete Repertory 2010), sighing, aversion to fruit, facial perspiration, etc. consistent with that medicine. Nux vomica also was a strong consideration, given his industry, irritability, fastidiousness, and chilliness, but his pleasing, yielding nature was an obstacle to its selection. In the end it was the pronounced elements of sympathy and a yielding, pleasing nature, coupled with the need for control (“The need for control over oneself and over one’s surroundings is tremendous, as is the need to keep order in the midst of chaos.”5), that decided the selection—Carcinosinum burnett, which was also well represented in the repertorization. (Carcinosinum burnett was selected, being the form of Carcinosinum represented in the above repertorization and, generally, in my estimation, the preferred Carcinosinum to prescribe absent more specific indications that might suggest another form of the nosode; such as, a past or family history of a very specific form of cancer; e.g., Carcinosinum uteri in the case of uterine cancer, or Carcinosinum co. in the case of multiple types of cancers in the history.)
Prescription: Carcinosinum burnett 10M, single dry dose.
Six weeks later: Patient reported that he responded very well—his sinuses and mood were improved, and his vision, which had been deteriorating was somewhat better and stable. Four months out from the first prescription, his ophthalmologist told him fluid was building in the retina again and he could anticipate another leak. Also, his sinuses were flaring up again.
Prescription: Carcinosinum burnett 10M, single dry dose.
One month after the foregoing prescription the patient reported that he felt great. His sinuses had improved, he was not feeling stressed, and his vision had been steadily improving. One year later, he reported that fluid was accumulating in his eye again; there’d also been some relapse of his sinusitis.
Prescription: Carcinosinum burnett 10M was again repeated.
Three months later, he reported a substantial improvement in his vision; his ophthalmologic exam was also much improved, so much so that his ophthalmologist advised him that he’d not require another exam for a year, a first for him. He was advised to get back in touch should he suffer a relapse of either condition, which to date, over ten years, he’s not found necessary.
Final comment and discussion
The correlation of the second patient’s CSCR pathology and his stressed, rather Type A personality6 and the known association of endogenous hypercortisolism due to stress with CSCR is notable.
Both of the cases presented demonstrate the considerable benefit that can follow a homeopathic medicine directed to the constitutional, for lack of a better term, terrain of the patient, irrespective of the presenting pathology, which offered no clues to any specific eye or sinusitis remedy. The characteristic symptoms in each case were those of the individual’s psychodynamics, in each case manifested as a unique stress response that corresponded to known patterns of mental-emotional distress as described in our homeopathic materia medica. This ability to correlate psychodynamics with a highly specific curative medicinal treatment is but one of the beauties of our unique medical discipline.
 About the Author: George Guess, MD, DABHM, is a family physician practicing homeopathy in the Charlottesville, Virginia area. He is an assistant editor of the “American Journal of Homeopathic Medicine,” Vice-President of the American Board of Homeopathic Medicine, and a trustee of the American Institute of Homeopathy. He holds a Diploma in Homeopathy from the Athenian School of Homeopathy (George Vithoulkas’s instructional program in Greece). Washington
About the Author: George Guess, MD, DABHM, is a family physician practicing homeopathy in the Charlottesville, Virginia area. He is an assistant editor of the “American Journal of Homeopathic Medicine,” Vice-President of the American Board of Homeopathic Medicine, and a trustee of the American Institute of Homeopathy. He holds a Diploma in Homeopathy from the Athenian School of Homeopathy (George Vithoulkas’s instructional program in Greece). Washington
References:
- Ahmed, Z, Shlamovitz, GZ, Muchatuta, M. Iritis and Uveitis. Medscape. https://emedicine.medscape.com/article/798323-overview#a8Updated: 03.09.2023
- Portnov, A. Acute Iridocyclitis. https://m.iliveok.com/health/acute-iridocyclitis_87869i15936.html. Updated: 11.10.2023 (Accessed 03.24.2023)
- Cowperthwaite, AC. A Text-Book of Materia Medica and Therapeutics, Characteristic, Analytical, and Comparative. Tenth Edition. Philadelphia. Boericke & Tafel. 1909. p. 170. “Heaviness in forehead; worse when reading or writing … Eyes. – Painful sensation, as if a small foreign body were in the eye (Acon.); sensation of sand. Profuse lachrymation (Euphr., Merc.) pupils dilated. Swelling and redness of the lids, with nightly agglutination (Aeth., Lyc., Merc., Puls., Sil., Sulph.); also in the mornings, eyes watery … Farsighted. Can see only one side of the object (Lyc.).]
- Weng, CY, Lim, J, Addara, J, et al. Central Serous Chorioretinopathy. Eye Wiki. American Academy of Ophthalmology. Dec 17, 2022. https://eyewiki.org/Central_Serous_Chorioretinopathy#Overview_of_Treatment
- Sankaran, R. Carcinosinum.The Soul of Remedies. Mumbai, India: Homeopathic Medical Publishers: Mumbai; 1997. (Accessed on ReferenceWorks.)
- Sharma, A. What is a Type A Personality? WebMD. November 09, 2021. www.webmd.com/balance/what-is-a-type-a-personality